1041
Views & Citations41
Likes & Shares
Background: Umbilical defects may cause technical problems for general surgeons in patients during laparoscopic cholecystectomy (LC) operations and may increase the incidence of incisional hernia.
Aim: The objectives of this study were to determine the optimal repair method for umbilical hernias during LC. Medical records of patients who had received simultaneous umbilical hernia repair with LC were investigated retrospectively.
Methods: Gall bladder stones was accompanied by umbilical hernia in 90 (6.1%) out of 1464 patients who underwent LC and umbilical hernia repair simultaneously in our hospital between January 2015 and July 2017.
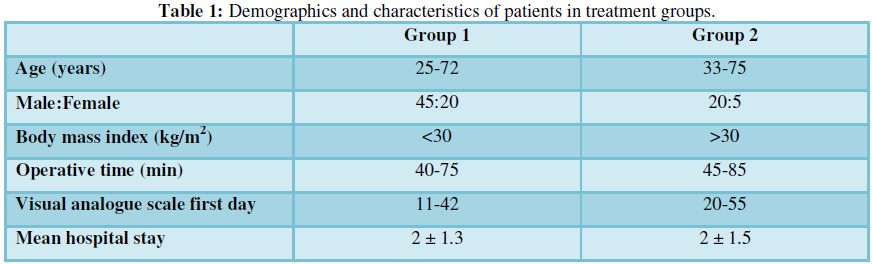
Results: LC was followed by umbilical hernia repair using primary suture in 65 patients (Group 1), progrip mesh repair in 25 patients (Group 2). Progrip mesh repair was performed in Mean body mass indexes (BMI) greater than 30.0 kg/m2 (Group 2).
Conclusion: The outcomes of the umbilical hernia repair with mesh after laparoscopic surgeries appear to be better for BMI greater than 30.0 kg/m2 than primary suture techniques in recurrence rates.
Keywords: Combined procedures, Laparoscopic cholecystectomy
INTRODUCTION
Laparoscopic cholecystectomy (LC) is “gold standard” for the treatment of cholelithiasis. Short length of hospital stay, immediate regaining of physical activity, low rates of postoperative pain, morbidity and mortality and good cosmetic outcomes make LC advantageous [1].
Umbilical hernias comprise 6% of all abdominal hernias in adults [2]. Several surgical methods have been used in the treatment of umbilical hernias. However, there is no consensus yet on the best method for umbilical hernia repair [3,4].
METHODS
With advancement in laparoscopic surgery a number of surgical procedures can be performed combined with laparoscopic cholecystectomy in a single surgery.
It is a retrospective clinical study performed in the department of surgery in İstanbul Medeniyet University Göztepe Educational Hospital Department of General Surgery.
These study exclusion criteria as follows, Patients with strangulated Umbilical Hernia(UH), abdominal malignity, severe cardiopulmonary disease, ascites and recurrent UH. Patient’s demographic data, operation time, hospital stay, complications, size of the defect, operation technic and recurrence rate were evaluated in hospital records database. We evaluate the safety and efficiency of those surgeries.
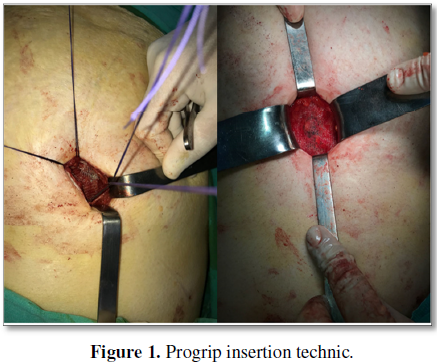
Under general anesthesia, we performed an incision at the level of the hernia. Hernia sac was isolated. It is inserted open laparoscopic port (Hasson Trocar) and prevents visceral injury beyond hernia sac. If the hernia size lower than 3 cm and BMI lower than 30 kg/m2 primary suture was performed.
RESULTS
1464 cholecystectomies were performed in the period from January 2015 to July 2017. Of these, 90 patients were performed combined surgery. The mean operative time was 45 min (range 35-125 min). The mean hospital stay was 2.1 days (range 1-3 days).
Median VAS pain scores measured on the postoperative first day in two groups. There were not statistically significant differences between two groups.
We had no recurrence of the hernias during our follow up period (range 6 months to 3 years).
Combined procedures provide patients with all the benefits of minimal invasive surgery and also give the benefit of single time anesthesia without adding to post-operative morbidity and hospital stay.
DISCUSSION
Many studies have investigated LC and its complications (incisional hernia from umbilical port) or UHR and its complications (recurrence rates). However, only a limited number of studies have reported short- and long-term outcomes of UHR performed simultaneously with LC in the same session. Prevalence of cholelithiasis accompanied by umbilical hernia varies between 4.7-18% (in our study, 6.1%) [8,9].
We have found no significant increase in the hospital stay or post-operative complications in the combined procedures. Combined procedures follow the trend of the more extensive procedure with regard to the postoperative course and postoperative pain.
In addition to the benefits of minimal access, patient gets the additional advantage of single hospital stay and single anesthesia exposure. Thus it is more convenient for the patient and also more cost effective.
In effect, procedures combined with laparoscopic cholecystectomy ‘kills two pathologies with one scope’.
SUMMATIVE DISCLOSURE
This article reports our experience with laparoscopic umbilical hernia suture repair when combined with another laparoscopic procedure.
DECLARATION OF CONFLICT OF İNTEREST
1. Berggren U, Gordh T, Grama D, Haglund U, Rastad J, et al. (1994) Laparoscopic versus open cholecystectomy: Hospitalization, sick leave, analgesia and trauma responses. Br J Surg 81: 1362-1365.
2. Lau H, Patil NG (2003) Umbilical hernia in adults. Surg Endosc 17: 2016-2020.
3. Wright BE, Beckerman J, Cohen M, Cumming JK, Rodriquez JL (2002) Is laparoscopic umbilical hernia repair with mesh a reasonable alternative to conventional repair? Am J Surg 184: 505-509.
4. Nguyen NT, Lee SL, Mayer KL, Furdui GL, Ho HS (2000) Laparoscopic umbilical herniorhaphy. J Laparoendosc Adv Surg Tech A 10: 151-153.
5. Jani K, Rajan PS, Sendhilkumar K, Palanivelu C (2006) Twenty years after Erich Muhe: Persisting controversies with the gold standard of laparoscopic cholecystectomy. J Min Access Surg 2: 49-56.
6. Wadhwa A, Chowbey PK, Sharma A, Khullar R, Soni V, et al. (2003) Combined procedures in laparoscopic surgery. Surg Laparosc Endosc Percutan Tech 13: 382-386.
7. Arroyo A, Garcia P, Perez F, Andreu J, Candela F, et al. (2001) Randomized clinical trial comparing suture and mesh repair of umbilical hernia in adults. Br J Surg 88: 1321-1323.
8. Nassar AH, Ashkar KA, Rashed AA, Abdulmoneum MG (1997) Laparoscopic cholecystectomy and the umbilicus. Br J Surg 84: 630-633.
9. Nguyen NT, Lee SL, Mayer KL, Furdui GL, Ho HS (2000) Laparoscopic umbilical herniorhaphy. J Laparoendosc Adv Surg Tech A 10: 151-153.
-
 Table 1
Table 1
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Alcoholism Clinical Research
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- Journal of Spine Diseases
- Journal of Cell Signaling & Damage-Associated Molecular Patterns
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- Ophthalmology Clinics and Research (ISSN:2638-115X)


